An advance health care directive is a document in which a person sets out his or her wishes regarding future health care decisions. These might include consent, refusal to consent, or withdrawal of consent for any care, treatment, service, or procedure to maintain, diagnose, treat, or provide for an individual’s physical or mental health.
Everyone should create advance directives, even if they are young and healthy! Continue to read below for an explanation of the different types of advance directive forms, then scroll down to locate the link to download or print your state's documents.
The advance directive allows you to make specific written instructions for your future health care in the event of any situation in which you can no longer speak for yourself. It outlines your wishes about life-sustaining medical treatment if you are terminally ill or permanently unconscious, for example.
None of us likes to think about how we would want healthcare delivered to us if we became critically ill or unable to communicate. But it is important to make these essential and very personal decisions – known as advance directives – before needing them.
More and more people are realizing the importance of having signed Advance Healthcare Directive forms prepared while you're in good health, in case they become unable to make decisions regarding your own healthcare.
The term 'advance directive' refers to your oral and written instructions about your future medical care in the event you are unable to express your medical wishes.
A Substitute Decision-Maker is an adult you choose and appoint in your Advance Care Directive to make decisions about your future health care, end of life, living arrangements and other personal matters when you are unable to make these decisions for yourself, whether for a short time only or permanently. The Substitute Decision-Maker(s) must sign the Form and accept their role.
Advance care planning allows you to make your voice heard so your wishes are followed. You can provide clarity and understanding among family members, your doctor and your health care team.
No one can predict the future. Terminal illness or accidents can strike at any moment, rearranging lives, altering priorities, and taxing health care plans. Advance health care directives can help to mitigate the fallout, for yourself and for your family.
An Advance Care Directive can be a useful tool for people to communicate instructions about future health care decisions. This factsheet explains the key legal principles on Advance Care Directives.
When we started our project, it was focused on advance directives for mental health care. That is still the major focus of our work. But we have expanded the website to include more about other types of advance care planning too. We hope you find the website helpful.
Although you may not like to think about it, there could be times in your life when you are unable to make a decision or properly communicate your wishes on how you would like to be cared for or treated. It could be for a number of reasons including an accident or mental health episode, or an illness or injury.
A health care directive is important if your attending physician determines you can't communicate your health care choices (because of physical or mental incapacity).
California Advance Health Care Directive Form (POA & Living Will), allows an individual to choose an agent to make healthcare decisions on his or her behalf in the event they can no longer make them.
You won’t need a lawyer to make your living will official, but most state do require signing the document in front of two witnesses. In many states, documents must also be signed in the presence of a notary public.
People of all ages may unexpectedly be in a position where they cannot speak for themselves, such as an accident or severe illness. In these situations, having an ACD assures that your doctor knows your wishes about the kind of care you want and/or who the person is that you want to make decisions on your behalf.
Use our attorney-drafted Advance Directive Form to grant a representative the power to make healthcare decisions on your behalf — ensuring you receive the right level of care.
You can use these documents to let your family and doctor know your decisions for health care if you become unable to decide for yourself. You can appoint someone you know and trust as your health care decision maker to ensure that your choice or decision is honored.
Advance directives allow for many choices. By completing an advance directive, you can identify treatments you want/don’t want, state your wishes about donating your body, organs and/or tissues at death, outline your wishes about burial and funeral arrangements, and even state your wishes about resuscitation.
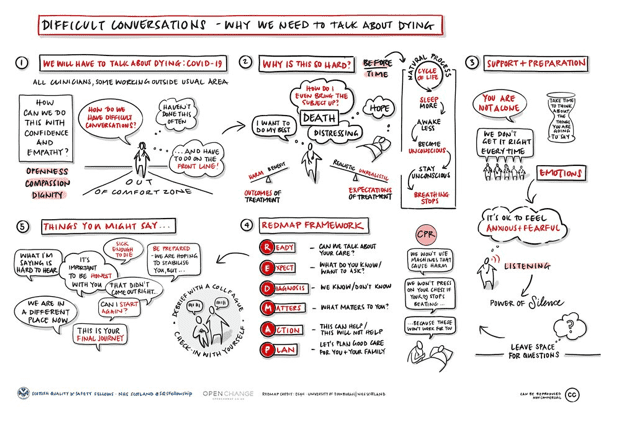
Difficult conversations – why we need to talk about dying
This
definition in use by the NQF and the Centers for Medicare and Medicaid
Services (CMS) must be combined with the continuity of communication
between care-givers in order to provide the highest standard in
palliative care.
PALLIATIVE CARE SHOULD BE AVAILABLE TO PEOPLE EARLIER
Many agreed that the benefits of palliative care should be available to people earlier in the progression of their disease.
From 2012 some studies even showed increased survival among those who received palliative care.
There was also a strong desire to move beyond cancer, the disease that had defined the approach of the hospice pioneers.
Areas of further palliative care specialisation began to appear – in cardiology, renal medicine, stroke, respiratory disease and neurological conditions.
The medical model of palliative care was gathering strength.
Likewise, domains of ‘general’, ‘specialised’ and ‘specialist’ palliative care came to be characterised according to the complexity of the problems encountered and the skills needed to address them.
Those who focussed on palliative care for older people (‘geripal’) stepped up to the plate and paediatric palliative care gathered its own momentum.
Palliative care according to setting (hospital or community based) came to be differentiated.
“Most
people who have a life-threatening condition can benefit from
palliative care, whether or not they are having active treatment.
Palliative care helps with personal, social and medical problems
associated with potentially mortal illness, especially pain and other
distressing symptoms. It assists families and carers and supports them
in bereavement. It uses skilled approaches from a trained team, but
often involves friends, family members and the wider community.
Palliative care improves wellbeing and in some instances has even been
shown to extend life”.
An
episode of admitted patient palliative care may comprise a single phase
or multiple phases, depending on changes in the patient's condition.
Phases are not sequential and a patient may move back and forth between
phases within the one episode of admitted patient palliative care.
Patient’s thoughts and feelings about illness, treatment, and care.
a. What do we need to know about you and your family to give you the best care?
b. How do you and your family best receive information?
c. What is most important to you right now? And as you think about the future? Is this different from what you perceive as important to your family?
Coping with emotions, functional changes, symptoms etc.
a. What have been the most significant changes in your life?
b. How does illness and symptoms affect your everyday life?
c. What does the future look like to you?
d. What substances (e.g., alcohol, marijuana, opioids, and cocaine) have you used or experimented with in the past? Have you ever used these substances to cope with unwanted feelings?
Cultural influences
a. How do you understand what is happening to your health?
b. What cultural or ethnic group do you identify with?7
c. What is your preferred language? What primary language is spoken at home?
d. Have you been able to maintain contact with family or friends from your country of origin? Have you any plans for visiting that family now or in the future?
e. (If appropriate to the patient’s awareness) Where is your preferred place of death?
Social context
a. Who is your family? Of origin and of creation?
b. How would you prefer to be addressed? Preferred pronoun?
c. Where do you live? Do you live alone or with others? Are there timeswhen you think about if/when you need more assistance at home andwhat thatmight look like?
d. Are you a veteran?
e. Are you currently employed?
Lived experience of illness, impact on self, others, and quality of life.
a. Do you worry about the financial impact or how your health expenses will be covered?
b. What has been the impact of this illness on your work and those important to you?
c. What or whom are you concerned about with regard to your health?
d. What have you shared about your illness with family and friends?
e. Who can help with decision making? Who do you go to when things get tough? Do you have a health care power of attorney or agent? Who might have copies of those documents?
f. Have you, or those close to you, managed serious illness before? Any recent losses?
g. (If appropriate to the patient’s prognostic awareness) Have you made funeral or after-death plans? Plans for cremation or burial here or in country of origin?
Suffering and the existential/spiritual domain
a. Are religious or spiritual beliefs or rituals important to you?
b. Are you being supported by a spiritual community? Does your illness allow you to still access this support? If not, can this support come to you—in person or through technology?
c. What brings you comfort?
d. How does this illness influence your thoughts and relationship to your god or a higher power?
"I have no financial relationships with manufacturers of commercial products or services. No conflicts of interests".
Whilst every effort is made to ensure the accuracy of this guide, the authors and organisations supporting it cannot accept liability for inaccuracies. Some recommendations are based on accepted practice, using medications outside their product licence, and not always with high quality evidence to support this. Individual clinical assessment and judgement is essential.
The use of this blog is voluntary and is intended to supplement.We make every effort to ensure the information in these pages is accurate and correct at the date of publication, but it is of necessity of a brief and general nature, and this should not replace your own good clinical judgement, or be regarded as a substitute for taking professional advice in appropriate circumstances.